Flat Foot
Mr Billy Jowett | Consultant Orthopaedic Surgeon
Expert Private Treatment for Adult Acquired Flatfoot Deformity
Struggling with Painful Flat Feet?
If you’ve been told you have flat feet and are experiencing pain, you’re not alone. As a consultant orthopaedic foot and ankle surgeon specialising in flat foot reconstruction, I see many UK patients who’ve been struggling with painful flat feet for years, often told to “just live with it.” But here’s what I want you to know: painful flat feet are different from simply having flat arches, and there are excellent treatment options available, both surgical and non-surgical.
I work primarily with private patients across the UK, accepting self-pay patients as well as those with private medical insurance including Bupa and AXA. You don’t need a GP referral to see me privately – you can book directly for an expert assessment.
What is a Flat Foot?
A flat foot is exactly as it suggests: on the inner aspect of the foot, there’s normally an arch stretching from the heel to the base of the toes. This ‘medial longitudinal arch’ develops through childhood, with the height varying amongst individuals. Some people never develop a medial arch, while others may develop a fallen arch as they age.

Flat Feet (Back)

Flat Feet (front)

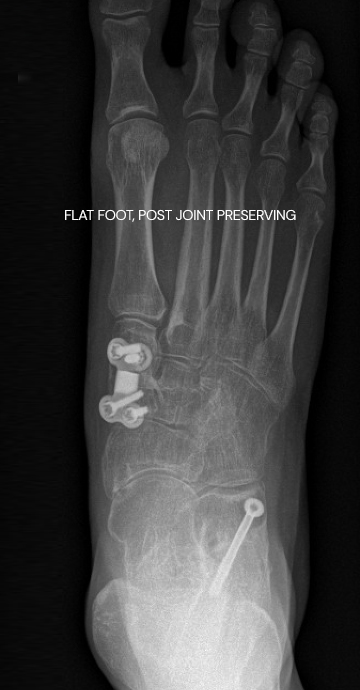
Flat Foot (Pre Op)

Flat Foot (Post Op)
Can Flat Feet Be Corrected in Adults?
This is one of the most common questions I’m asked, and the answer is yes – adult flat feet can absolutely be corrected. The type of correction depends on the cause of your flat foot and how far the condition has progressed. I offer both joint-preserving flat foot reconstruction and fusion procedures, depending on what’s most appropriate for your specific situation.


What is Adult Acquired Flatfoot Deformity?
Adult acquired flatfoot deformity (AAFD), also known as posterior tibial tendon dysfunction (PTTD) or ‘fallen arches’, is quite different from the flat feet you might have been born with. This condition develops later in life, and I tend to see two patterns in my UK private practice:
The first type: Patients who have always had slightly flat feet, but suddenly they’ve started to hurt and collapse further. This happens when the supporting structures can no longer cope with the strain they have been under for years.
The second type: Patients who have had relatively normal feet, but then the medial longitudinal arch starts to lower. This is more common in middle-aged women, possibly related to hormonal changes and ligamentous laxity.
Both presentations share a common feature: the failure of a critical tendon called the tibialis posterior tendon. I feel these patients can get a rather raw deal, because this condition can go undiagnosed and therefore untreated and more recently there has been a move for podiatrists (who provide the mainstay of treatment of the early stages of the acquired adult flat foot) in the NHS to focus on the treatment of diabetic feet and therefore access to orthotics has become more difficult.
Why Do Flat Feet Develop in Adults?
Understanding what’s happening in your foot helps explain why treatment works. The main cause is:
Do I Need Flat Foot Surgery? Recognising Flat Feet Symptoms and Signs
Not all flat feet need treatment, although one could make an argument that it would be sensible to wear supportive shoes with or without supportive insoles (orthotics) if you have flat feet to reduce the stress on the tibialis posterior tendon to reduce the chance of problems with the tibialis posterior tendon.
Formal treatment is required if you develop pain particularly if it is affecting your function/ day-to-day life.

Flat Foot Treatment: Orthotics vs Surgery – Which Do You Need?
I always start with conservative treatment when possible. Many patients can manage their symptoms successfully without surgery, and it’s important to explore these options thoroughly before considering operative treatment.
When Should You Consider Flat Foot Surgery?
This is where I need to be philosophical with you. The timing of surgery comes down to your symptoms rather than some arbitrary staging system. Even if you have advanced flat foot deformity, if you can manage with orthotics and bracing and maintain your quality of life, there may be no rush for surgery.
However, if conservative measures aren’t controlling your symptoms adequately, or if the deformity has progressed beyond what bracing can manage, then it’s time to consider surgery.
Key indicators include:
Important considerations:
So, while I don’t believe people necessarily “leave it too late,” I do think timely assessment is important. Even if you’re not ready for surgery, getting proper orthotics fitted can prevent the progression that would limit your surgical options later.

What Does Flat Foot Reconstruction Surgery Involve?
As one of the UK’s specialist surgeons for flat foot reconstruction, let me be direct about one thing: simple tendon procedures alone, in my opinion, don’t work for established flat feet. Some surgeons transfer tendons to shore things up, but here’s why I take a more comprehensive approach:
The Standard Reconstruction: Tibialis Posterior Tendon Reconstruction (Joint-Preserving Surgery)
For most flat feet that haven’t become rigid, I perform what’s called a joint-preserving flat foot reconstruction. This is the gold-standard treatment for adult acquired flatfoot deformity in the UK and typically involves some or all of these four elements:
This might sound like the “smorgasbord” approach, but each element addresses a specific mechanical problem. The recovery from adding a Cotton osteotomy or calf muscle lengthening doesn’t significantly change the overall rehabilitation timeline.
Triple Arthrodesis Flat Foot Surgery UK
If your flat foot has become rigid, or if arthritis has developed in the talonavicular, subtalar, and calcaneocuboid joints, I can’t preserve the movement in these joints. Instead, I perform a triple arthrodesis, fusing these three joints in a corrected position, the joint surfaces are prepared in a way that should allow them to join together (fuse) (and removes any arthritis present in these joints), and they are fixed typically with screws and staples.
While this eliminates some motion, it restores proper alignment and eliminates pain from arthritic joints. Many patients function very well after triple arthrodesis and find the trade-off of some lost motion for pain relief and stability to be well worthwhile.

Triple Arthrodesis (Pre Op)
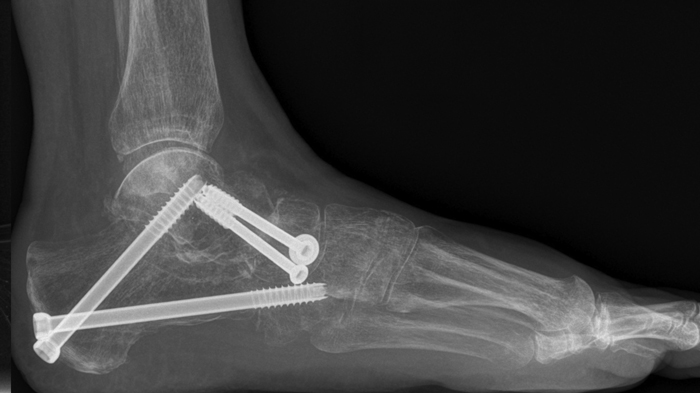
Triple Arthrodesis (Post Op)
Advanced Cases with Ankle Arthritis
In the most advanced cases where ankle arthritis has developed alongside the flat foot deformity, I may need to perform ankle replacement surgery at a separate sitting after performing the flat foot correction. This addresses both problems in the corrected foot position.
Tarsal Coalition Surgery
This is a separate topic as it is not part of the classical acquired adult flat foot deformity. If there’s a coalition (link between the bones) present that has become painful and hasn’t settled with non-operative management sometimes the coalition can be excised, in other situations the heel bone is reset (calcaneal osteotomy: see above) to decrease the forces causing stress on the coalition.
What Our Patients Say
“Mr Jowett talked and listened to me prior to my operation and afterwards, showing empathy and understanding. He put me at ease and talked about things that were worrying me. Since my bunion operation I have had no pain and my foot has healed remarkably well. The scar hardly shows and I have now gone back to walking and exercise classes. He is professional and a great surgeon. I highly recommend him to anyone.”
Understanding Flat Foot Stages
You may have heard about staging systems for flat feet (typically stages 1-4). While these don’t dictate the timing of my surgery recommendations – symptoms do that – they do influence which surgical procedure is most appropriate:
Stage 1: Tibialis posterior tendinopathy without deformity
Stage 2: Flexible flat foot deformity (further divided into 2a, 2b and 2c based on degree of forefoot deformity and correctability) – treated with joint-preserving reconstruction
Stage 3: Rigid flat foot or one with arthritis in the triple joint complex (the subtalar, talonavicular and calcaneocuboid joint, those under and just in front of the ankle that work together to move the back of the foot inwards and outwwards) – requires triple arthrodesis
Stage 4: Flat foot with ankle arthritis – needs foot reconstruction combined with ankle replacement
Various classification systems exist, and new ones are always being proposed, but this framework gives you a sense of how progression affects treatment options.

How Long is Recovery After Flat Foot Surgery, and When Can I Walk Again?
I believe in being realistic with my patients about flat foot surgery recovery time. This isn’t about creating a bionic foot – it’s about pain relief, improved function, and preventing further deterioration. Here’s what you can expect during your flat foot reconstruction recovery in the UK:
What Are the Risks and Complications of Flat Foot Reconstruction?
As with any surgical procedure, it’s important to understand the potential risks. I believe in having honest conversations with my patients about what could go wrong, even though the vast majority of my flat foot reconstruction surgeries go smoothly without complication.

What is the Best Flat Foot Surgery UK?
Patients often ask me what the “best” flat foot surgery is. The truth is, there’s no single answer – the best flat foot surgery for you depends entirely on your specific condition, the stage of your deformity, your activity goals, and whether your joints are still flexible or have become rigid.
What Makes It “Best”?
Beware of surgeons offering isolated tendon transfers without bone realignment procedures – in my experience these have high failure rates. Comprehensive reconstruction with calcaneal osteotomy is essential for lasting results.
My Approach to Flat Foot Problems: Specialist UK Orthopaedic Foot and Ankle Surgeon
As a foot specialist, I provide expert assessment and treatment for flat foot problems across the UK, with a particular focus on serving patients across the South Downs (e.g Hampshire and West Sussex) as well as Jersey.
I perform a comprehensive reconstruction when needed, addressing all mechanical problems simultaneously rather than taking a piecemeal approach. I offer the full range of modern techniques, from joint-preserving reconstruction and fusion surgery, with clear, honest communication about all your options.
I work primarily with private patients who want rapid access to specialist care without NHS waiting times. I accept private medical insurance (Bupa, AXA, Aviva, Vitality, WPA, and others) as well as self-funding patients. You don’t need a GP referral to book a consultation.
Whether you’re seeking a second opinion, exploring surgical options, or need expert orthotic guidance, I take time to understand your individual circumstances, activity goals, and treatment preferences. I work with local physiotherapists to ensure comprehensive rehabilitation support throughout your recovery.

Frequently Asked Questions About Adult Flat Foot Surgery
What Our Patients Say
“Mr Jowett talked and listened to me prior to my operation and afterwards, showing empathy and understanding. He put me at ease and talked about things that were worrying me. Since my bunion operation I have had no pain and my foot has healed remarkably well. The scar hardly shows and I have now gone back to walking and exercise classes. He is professional and a great surgeon. I highly recommend him to anyone.”
Take the Next Step Towards Pain-Free Walking
If you’re living with painful flat feet, don’t accept it as something you simply have to put up with. Early specialist assessment can prevent progression, protect your joints, and give you clarity about your treatment options — whether that’s expert orthotic guidance or advanced reconstructive surgery.
You don’t need a GP referral to book privately. I welcome both self-pay and insured patients, including Bupa, AXA, Aviva, Vitality and WPA.