Bunion Surgery (Hallux Valgus)
Mr Billy Jowett | Consultant Orthopaedic Surgeon
Private bunion clinics in Southampton, Portsmouth and Chichester | Appointments typically available within 1–2 weeks
Bunion Surgery Explained: Making the Right Decision for Your Feet
If you have been told you have a bunion, or if you have noticed a bony lump forming at the base of your big toe, you are far from alone. Bunions are one of the most common foot conditions I treat, and also one of the most misunderstood. Many patients arrive having been told they simply need to ‘have the bump removed’, or having seen adverts for quick keyhole procedures. The reality is more nuanced, and understanding the decision-making involved will help you feel confident about whichever path is right for you.
I offer private bunion surgery at clinics across the South of England, including Southampton, Portsmouth and Chichester. If you would like to discuss your options, you can book a consultation directly online.
What Our Patients Say
“Mr Jowett talked and listened to me prior to my operation and afterwards, showing empathy and understanding. He put me at ease and talked about things that were worrying me. Since my bunion operation I have had no pain and my foot has healed remarkably well. The scar hardly shows and I have now gone back to walking and exercise classes. He is professional and a great surgeon. I highly recommend him to anyone.”
What exactly is a bunion?
The word ‘bunion’ is often used loosely, but the dictionary definition is a painful swelling on the first joint of the big toe. A classical bunion describes the prominent bony area that develops at the base of the big toe in association with the big toe being angulation towards the other toes. The medical term for this deformity is hallux (Latin for big toe) valgus (angulation away from the midline).
The bump itself is not new bone growing — it is the head of the first metatarsal (the long bone leading to the big toe) becoming exposed as the toe moves out of position. As the deformity develops, the tendons that bend the toe up and down no longer run up and down over the centre of the joint, they run on the lesser toe side of the joint, gradually pulling the great to further out of alignment. Left untreated, bunions tend to worsen over time.

Why do bunions develop?
Bunions are thought to develop for two main reasons: genetics and footwear. They tend to run in families, and populations around the world who never wear shoes have a lower incidence. A combination of genetic predisposition and narrow or pointed shoes is probably the most common cause.
In some people, the underlying joint between the first metatarsal and the foot — the first tarsometatarsal (TMT) joint — is naturally more mobile than it should be. This instability can gradually allow the medial arch to collapse and can make the great toe more likely to become angulated, and is an important factor in how I approach surgery.

What symptoms do bunions cause?
The most common problem is pain due to the prominent bone rubbing on shoes. But bunions can also cause:
It is also important to consider other symptoms such as:
As these may suggest that you do not just have a simple bunion, but there may be some associated arthritis in the joint at the base of the toe.
It is worth noting that the size of a bunion does not always reflect the level of pain. Some people have a very large deformity but minimal discomfort; others have a modest angulation that significantly affects their day-to-day life. My approach is always to treat your symptoms, not the X-ray.
When should you have bunion correction surgery?
This is one of the questions I am asked most often. Surgery should be driven by your symptoms and how much they affect your life — not by the appearance, not because someone has told you it looks bad or because you have been told that you have a bunion on a X-ray.
Surgery is worth considering when:
What I caution against is having surgery too early, before the symptoms genuinely warrant it. Equally, I see people who have waited so long that secondary problems with the smaller toes have developed, making the operation more complex. There is no universal right time — it is a conversation we have together, and I can help you make the decision as to what is the most appropriate treatment based on your specific situation.
What is the best type of bunion surgery?
The honest answer is that there is no single ‘best’ bunion treatment. The right procedure depends entirely on where you have a mild, moderate or severe bunion deformity, the stability of the underlying joints, and whether any arthritis is present. I use three main approaches, and the choice between them is made carefully with you in advance — not on the operating table.
What about the smaller toes and the rest of the front of the foot?
Around 30% of my patients having bunion operation also need some surgery to the second toe or other areas of the front of the foot at the same time. When the great toe is angulated its ability to take weight through it is affected altering load distribution across the forefoot, and the second toe is often the first to suffer as a result.
The problems I look for follow a recognisable progression: inflammation (synovitis) of the joint at the base of the second toe, if this is left untreated, a plantar plate tear can develop, where the ligament holding the toe down at the base of the toe tears and the toe begins to lift leading to a hammer toe. Techniques for repairing the plantar plate have been available since around 2010. If the toe remains hammered for a period, the first joint in the toe that bends over becomes fixed, i.e. the joint cannot be straightened with pressure. This sort of a fixed flexion deformity requires a different operation from a flexible hammer toe correction, involving removal of the joint that is bent over, correcting its position and stabilizing it with an implant or wire, often the tendon that pulls the toe up needs to be lengthened and sometimes a Weil osteotomy, to shorten the bone at the base of the toe to allow the great toe to drop into position, is required.
An important point: if your big toe is angulated — even if it is not painful — and you want your second toe corrected, sometimes I need to address the bunion at the same time to provide enough room for the second toe to sit back in the correct position. If there is not enough space for the second toe to sit between the great and third toes once it has been straightened, due to the angulation of the great toe, it will then sit on top or under the great toe causing continued pressure against shoes.
The abnormal pressure distribution through the front of the foot due to ana angulated and/ or painful great toe can also lead to other problems such as an irritated pocket of fluid and/ or nerve around the nerve between the metatarsal heads (at the base of the toes) known as a Morton’s neuroma. This can often need treating at the same time as surgery to correct the bunion. Often we will try an injection which often settles the pain and inflammation, but if the pain persists, we can remove the nerve at the same time as correcting the bunion. Although this usually causes numbness between the toes, patients usually find this a reasonable trade off if the pain is removed at the same time. It is important to remember that not all Morton’s neuromas cause pain.
What Our Patients Say
“I suffered for a long time in a lot of pain with a bunion and a shortening of ligaments in another toe. Mr Jowett operated on both of these and I am no longer in pain and back on the golf course pain free.”

What about minimally invasive bunion surgery?
Minimally invasive bunion surgery — sometimes referred to as keyhole bunion surgery or MICA (Minimally Invasive Chevron and Akin osteotomy) — is attracting a great deal of patient interest, and one can understand why.
My main concern with some minimally invasive procedures is the limited direct visual access to the bones during surgery, essentially the surgery is done by feel and X-ray control. This is different from other keyhole surgery eg. arthroscopic surgery to joints or laparoscopic surgery to the abdominal contents eg. bowel or to the kidney. In these cases, a camera is inserted and the picture it provides is displayed on a television screen giving the surgeon a magnified view of what they are operating on. Keyhole bunion surgery is the exact opposite; it relies on the surgeon having less visibility and therefore there is a significant learning curve i.e. the number of cases the surgeon has to perform before becoming proficient at the procedure.
Also, some minimally invasive techniques also rely on shortening the first metatarsal to achieve realignment — and a shortened first metatarsal increases the risk of overloading the second toe and causing new pain under the ball of the foot. This was well recognised as a problem with older operations such as Wilson’s osteotomy, which also relied on shortening to allow the correction.
If a minimally invasive bunion removal surgery appeals to you, I am happy to discuss whether it would be appropriate for your specific deformity at your consultation
Your questions answered
The cost of private bunion surgery in the UK depends on which procedure is needed and whether any additional corrections — such as a second toe repair — are required. The table below gives a guide to typical costs as a self-funding patient at my clinics.
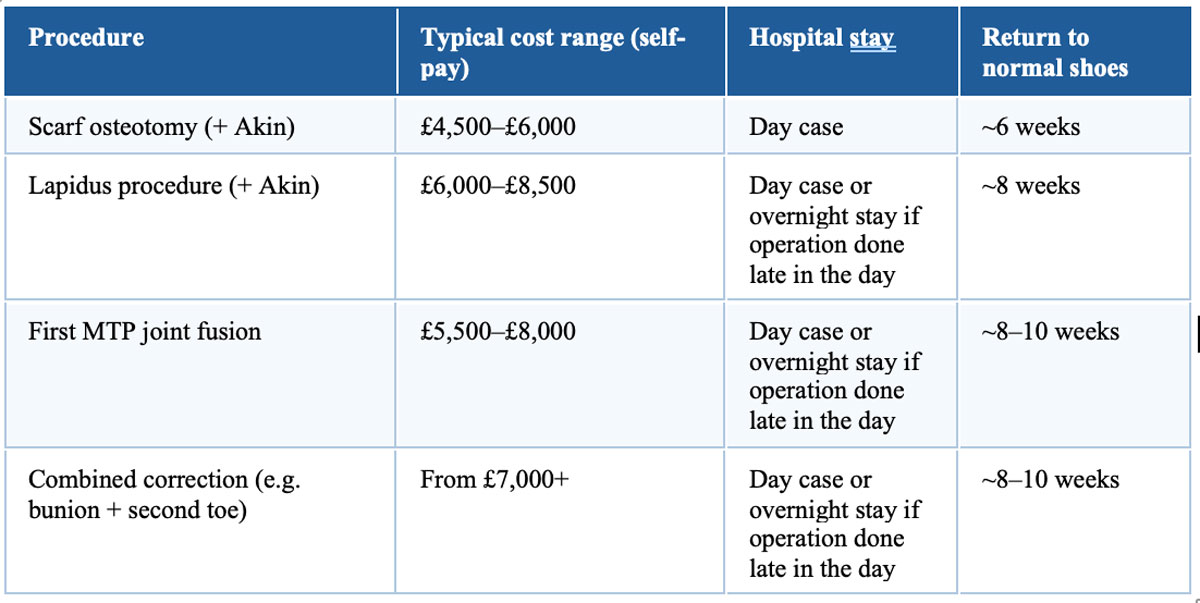
These figures are a guide; your surgeon’s fee, anaesthetist’s fee, and hospital facility costs are included in the package price quoted to you before any treatment begins. There are no hidden charges.
If you have private medical insurance — including Bupa, AXA Health, Vitality, or most other major insurers — bunion surgery is typically covered, subject to your policy terms and any excess. I am recognised by all major insurers and hold Platinum Consultant status with Bupa. My secretary can confirm your coverage and provide a full cost breakdown ahead of your consultation.
Recovery depends on which procedure you have had and your own body’s healing. As a practical guide:
- Scarf osteotomy: post-operative shoe for four to six weeks; back in normal shoes from around six weeks; swelling may persist for up to three months.
- Lapidus procedure: plaster for four weeks, post-operative shoe for a further four weeks; normal shoes from around eight weeks; full recovery four to six months.
- First MTP fusion: similar timeline to Lapidus; the foot can take several months to feel completely settled.
Return to driving is typically six to eight weeks after surgery, or sooner for left-foot operations in an automatic car, subject to your insurance policy and your ability to perform an emergency stop. Most people are back to normal daily activities within three to four months.
Most patients are pleasantly surprised. You will have a general anaesthetic, and local anaesthetic is placed around the ankle at the time of surgery, so you will wake up comfortable. The first 24 to 48 hours at home can be uncomfortable once the local anaesthetic wears off, but regular pain relief keeps this very manageable for the vast majority of people. Taking pain relief regularly from the start — rather than waiting until you are in pain — makes a significant difference to those early days.
Longer term, a degree of swelling and mild aching is normal for several weeks, but sharp pain should not be a feature of recovery, and most patients are surprised by how functional they feel.
If you have had bunion surgery elsewhere and are not happy with the result — whether the deformity has recurred, the pain has persisted, or a new problem has developed — I am very happy to see you for a second opinion. Revision bunion surgery is technically demanding, and it is an area where I have particular experience.
I also see patients who are unsure whether they need surgery at all. In my experience, many people with mild or moderate deformities can be managed well without an operation, and surgery done before the symptoms genuinely warrant it can leave someone worse off than if they had waited. If you have been told you need surgery and want a clear, honest assessment, please do get in touch.
My interest in complex and revision bunion cases stems from my fellowship training, including spending time with Professor Sigvard Hansen in Seattle — one of the founding fathers of foot and ankle surgery, and a renowned advocate of understanding and correcting the underlying cause of deformity rather than simply addressing the visible bump.
My approach: symptoms first, scans second
I want to end with something I say to almost every patient who comes to see me for a bunion assessment. People often ask: ‘Do I need an operation? What does my scan show?’
The honest answer is that the decision is based on your symptoms and what I find when I examine you — not the imaging. Scans and X-rays help me plan the surgery and choose the right technique; they are not the reason for doing it. I have seen patients with alarming-looking X-rays who do not need surgery at all, and patients with seemingly modest changes who are in significant pain and clearly benefit from an operation.
The right operation, for the right patient, at the right time. That is what guides everything I do.
What to expect at your consultation
At your first appointment, I will:
I will not recommend surgery unless I believe the benefits clearly outweigh the risks for you specifically. And I will not perform any operation that we have not agreed upon together in advance.
I hold private bunion clinics in Southampton, Portsmouth, Chichester and Jersey. You can book a consultation online, or my secretary is happy to help if you would prefer to call.
Take the next step towards pain-free walking.
If your bunion is limiting your comfort, footwear, or quality of life, I would be very happy to help. Book a consultation with Mr Billy Jowett at one of his private clinics in Southampton, Portsmouth or Chichester — appointments are typically available within 1–2 weeks.